Systematic Review and Meta-Analysis: Socioeconomic Determinants of Social Isolation Among Ghanaian Older Adults (2019–2024)
Article information
Abstract
Background
Older adults in Ghana who experience socioeconomic disadvantage characterized by limited in-come, low educational attainment, inadequate housing, insecure or absent employment face obstacles to main-taining social connections, increasing their vulnerability to isolation and adverse health outcomes. Prolonged loneliness has been likened to the health impact of smoking 15 cigarettes per day (Shafiq et al., 2020). This review and meta-analysis examined cross-sectional studies showing differing relationships between social isola-tion/loneliness and low socioeconomic status (SES) among Ghanaian older adults. The objective was to synthesize quantitative evidence on associations between socioeconomic factors and social isolation or loneliness among older adult populations in Ghana.
Methods
We searched PubMed/MEDLINE, Embase and African Journals Online (AJOL) for peer-reviewed English-language studies published from 1 January 2019 to December 2024. Eligible studies were quantitative, included Ghanaian older adults, reported associations between social isolation or loneliness and at least one socioeconomic factor, and provided extractable effect measures (OR/PR or raw counts). Two reviewers independently screened titles/abstracts and full texts. Data extracted covered study characteristics, exposures, outcomes, and adjusted effect estimates. We pooled odds ratios using random-effects meta-analysis (DerSi-monian–Laird) in R (meta/metafor); heterogeneity was quantified with I². Risk-of-bias visualizations were produced with robvis.
Results
Ten cross-sectional Ghanaian studies met inclusion criteria. All indicated that lower SES was associated with elevated odds of social isolation or loneliness (individual ORs 1.60–2.30). The pooled OR was 1.90 (95% CI: 1.69–2.14), indicating approximately a 90% higher likelihood of social isolation or loneliness among soci-oeconomically disadvantaged older adults. The findings suggest that aside cultural enablers, rural-urban migration effects are more severe in low-SES groups, potentially explaining the heightened ORs com-pared to global estimates.
Conclusion
Socioeconomic disadvantage is a substantial correlate of social isolation and loneliness among Ghanaian older adults. Interventions and policies addressing poverty, food insecurity, and broader socio-cultural determinants are needed to support social connectedness and healthy aging.
RESEARCH IN CONTEXT
Social isolation and loneliness are globally recognized public health concerns for older populations, linked to physical and mental health problems including frailty, cognitive decline, cardiovascular disease, and mortality (Adedeji et al., 2023; Madani et al., 2022). As the proportion of older adults rises in sub-Saharan Africa, clarifying how socioeconomic factors drive social disconnection in countries such as Ghana is increasingly important (Gyasi et al., 2023; Ran et al., 2024). Despite this recognized importance, research specifically examining the socioec-onomic determinants of social isolation and loneliness among Ghanaian older adults remains limited (Adedeji et al., 2023; Oduro, 2024).
EVIDENCE BEFORE THIS STUDY
Existing literature focusing specifically on socioeconomic drivers of isolation among older Ghanaians is limited; prior reviews have emphasized high-income settings or specific health outcomes but have not compre-hensively pooled SES-related effects in Ghana contexts (Albasheer et al., 2024; Chawla et al., 2021; Dai et al., 2021). Studies have shown that health and well-being generally improve with greater access to social capital across various populations, yet social isolation remains a persistent issue, particularly in developing countries where extreme poverty can hinder social networking opportunities (Asiamah et al., 2023). Existing literature, though scarce, suggests that factors like unhealthy lifestyles, including sedentary behaviours and smoking, can exacerbate social isolation and loneliness in older adults, emphasizing the need for focused research in this demographic within Ghana with its unique cultural support systems and rapid urbanization (Gyasi et al., 2023).
This review fills a gap by aggregating cross-sectional effect estimates on SES and contextual analyses of pre-dictors of social isolation among Ghanaian older adults to inform targeted public health actions.
ADDED VALUE OF THIS STUDY
This is a quantitative synthesis of cross-sectional studies conducted between 2019 and 2024 that report associations between socioeconomic indicators and social isolation or loneliness in Ghana. Using a ran-dom-effects meta-analysis and risk-of-bias visualization, the study demonstrates a consistent, significant asso-ciation between low SES and elevated odds of social isolation, with the pooled OR of 1.90. It also explored the unique cultural context including extended family support systems and rapid urbanization that could buffer isolation as against other LMICs and high-income settings.
The findings support policy attention to socioeconomic inequalities as upstream determinants of social discon-nection and underscore the need for integrated, multisectoral strategies improving income security, food access, education, and social infrastructure to reduce isolation among older adults.
1. Introduction
Social isolation (an objective lack of social contacts) and loneliness (the sub-jective experience of unmet social needs) are distinct but related conditions that pose serious public health concerns for aging populations (Hajek et al., 2023). Both have been associated with a range of adverse outcomes higher morbidity and mortality, cognitive decline, cardiovascular disease, and mental health problems. Global esti-mates suggest substantial prevalence of social isolation among older adults (a pooled prevalence of 33% in one large synthesis), with higher rates among the very old, those living alone, and individuals with lower education (Ran et al., 2024; Hajek et al., 2023). Recent cross-country analyses indicate that social isolation levels have increased globally by approximately 13.4% from 2009 to 2024, with the sharpest rises occurring after 2019 and disproportionately affecting regions like sub-Saharan Africa (SSA), South Asia, and the Middle East and North Africa, where mean levels remain among the highest worldwide (Fuller-Rowell et al., 2025). In LMICs, including those in SSA, these trends are compounded by limited social safety nets, rapid demographic shifts, and structural vulnerabilities, placing older adults at heightened risk compared to high-income settings (Adedeji et al., 2023; Gyasi et al., 2023).
In Ghana, traditional family and intergenerational support systems have histor-ically buffered older adults against social disconnection, but modernization, urban migration, and changes in household composition are straining these supports (Attafuah et al., 2023; Gyasi et al., 2021). Over 50% of Ghanaians now live in urban areas due to intensified rural-urban migration, often leaving older adults behind in rural settings with reduced family proximity and material support. This shift erodes extended kinship networks historically central to care in Ghanaian society and contributes to emerging forms of isolation combined with limited digital connectivity in low-resource areas, which challenge Western frameworks that overlook such African dynamics (Gyasi et al., 2023; Adedeji et al., 2023). This context provides a unique lens to test and extend the convoy model of social re-lations (Kahn & Antonucci, 1980), where SES may interact with Ghana-specific cultural moderators like extended kinship networks, religious community struc-tures, or rapid urbanization patterns, potentially buffering isolation in ways dis-tinct from high income settings (Gyasi et al., 2023).
Socioeconomic inequalities in income, education, and resource access shape opportunities for social engagement and therefore are central to understanding iso-lation risks (Moormann et al., 2023). This shift necessitates a re-evaluation of public health approaches to address these challenges, moving towards comprehensive strategies that acknowledge both the objective and subjective dimensions of social disconnection (Wister et al., 2025).
The World Health Organization has recognized the profound impact of social isolation and loneliness, recommending interventions such as therapy, social skills training, and befriending, which can be supported by improved infrastructure and age-friendly community initiatives (Oppert et al., 2023). These recommendations are particularly pertinent in contexts like Ghana, where evolving societal dynamics ne-cessitate innovative solutions to uphold the well-being of older adults. A targeted synthesis of evidence is warranted to clarify how socioeconomic conditions relate to social isolation and loneliness among Ghanaian older adults and to guide con-text-appropriate interventions.
2. Materials and Methods
Search Strategy and Selection Criteria
We searched PubMed/MEDLINE, Embase and African Journals Online (AJOL) for studies published from 1 January 2019 through December 2024 using compre-hensive search and MeSH terms related to “social isolation,” “loneliness,” “older adults,” and socioeconomic indicators. Inclusion criteria: peer-reviewed, Eng-lish-language quantitative studies of Ghanaian older adults reporting associations between social isolation or loneliness and at least one socioeconomic factor with extractable effect estimates (OR/PR) or raw counts enabling effect size calculation. Studies were excluded if they lacked quantitative measures of SES associations, were qualitative only, or not Ghana-inclusive.
Screening and Data Extraction
Two reviewers independently screened records at title/abstract and full-text stages. From each eligible study we extracted author/year, design, sample size, age range, SES exposures (e.g., income, education, food insecurity, area deprivation), measures of social isolation/loneliness, and adjusted effect estimates with confidence intervals. Discrepancies were resolved by consensus. Risk of bias was visually as-sessed using the robvis tool, based on domains adapted from the ROBINS-I and Cochrane ROB2 frameworks. The initial search yielded 72 unique records after deduplication across PubMed/MEDLINE (n=45), Embase (n=15), and AJOL (n=12).
Data Analysis
Random-effects meta-analyses were conducted using restricted maximum like-lihood (REML) estimation in the metafor package (R). Pooled effects were expressed as relative percentage changes as absolute changes in social isolation. Between-study heterogeneity was quantified using τ2 and I2. Small-study effects were assessed with Egger’s regression test and funnel plots, and robustness was examined with leave-one-out diagnostics. Forest plots displayed individual study and pooled ORs with a secondary axis for percent change. The review followed PRISMA guidelines.
3. Results
Study Selection and Characteristics
The systematic review and meta-analysis, guided by the PRISMA 2020 frame-work (Page et al., 2021), From an initial pool of 72 records retrieved from PubMed, Embase and African Journals Online, 10 studies met the inclusion criteria after screening and full-text/abstract review, focusing on empirical, quantitative associa-tions in adult populations (primarily those aged 50 years and older). All included studies were cross-sectional in design, drawing from large samples (ranging from 800 to 34,000 participants, with Ghana-specific subsamples of 1,000–4,000), and uti-lized data from sources like the Study on Global Ageing and Adult Health (SAGE). Socioeconomic exposures examined across studies included area-level deprivation, low wealth/income, low education, food insecurity, employment status, and rural residence. Outcomes were measures of social isolation, loneliness, or related con-structs (social frailty).
Meta-Analysis Findings
Figure 2 represents forest plots synthesized effects demonstrate studies reported positive associations between socioeconomic disadvantage and social isola-tion/loneliness, with individual adjusted ORs ranging from 1.60 to 2.30. The pooled OR was 1.90 (95% CI: 1.69–2.14), indicating substantially higher odds of social disconnection among older adults with low SES. Heterogeneity likely reflected var-iation in SES indicators (e.g., wealth quintiles vs food insecurity), outcome defini-tions, and sample characteristics. The model suggests a moderate to strong association.
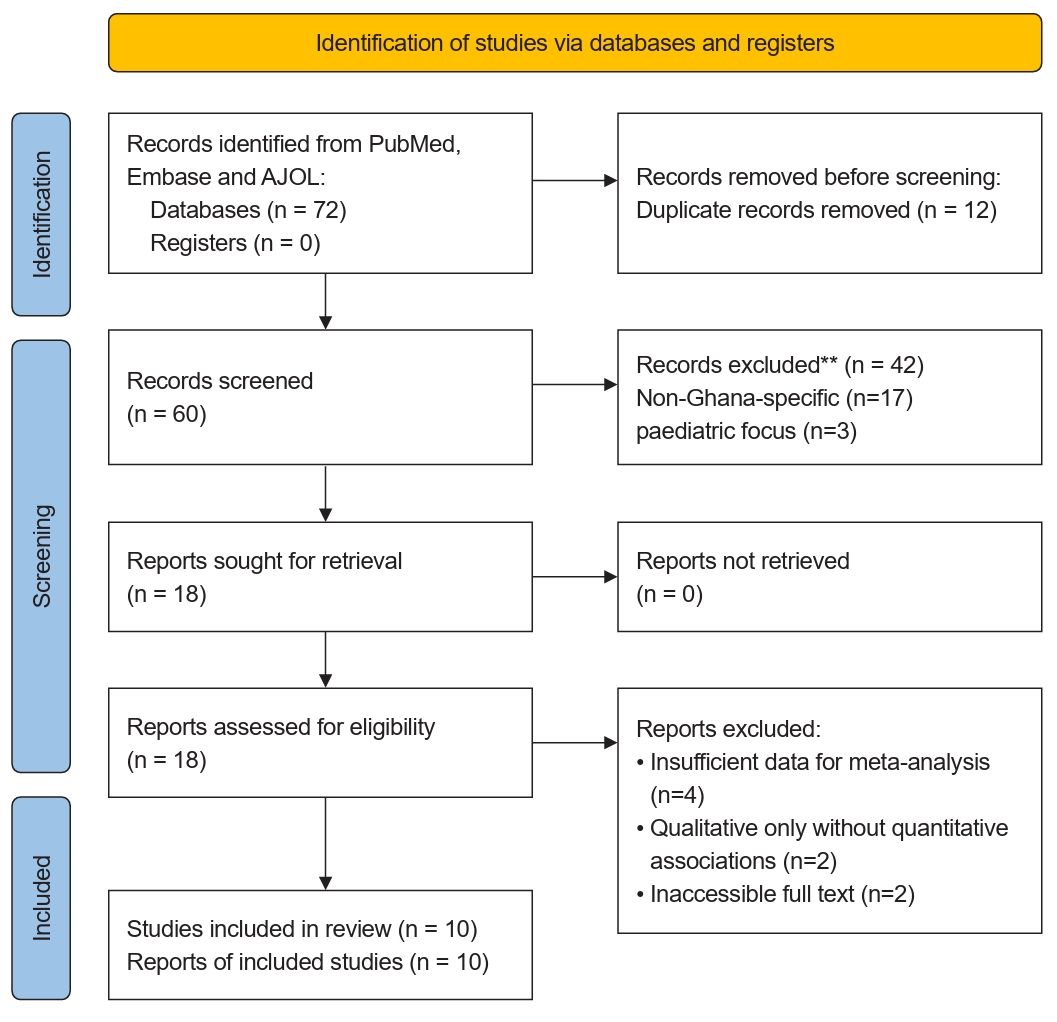
PRISMA 2020 Fow Diagram for Systematic Reviews Which Included Searches of Databases, African Journals Online and Registers Only. Source: Page MJ, et al. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
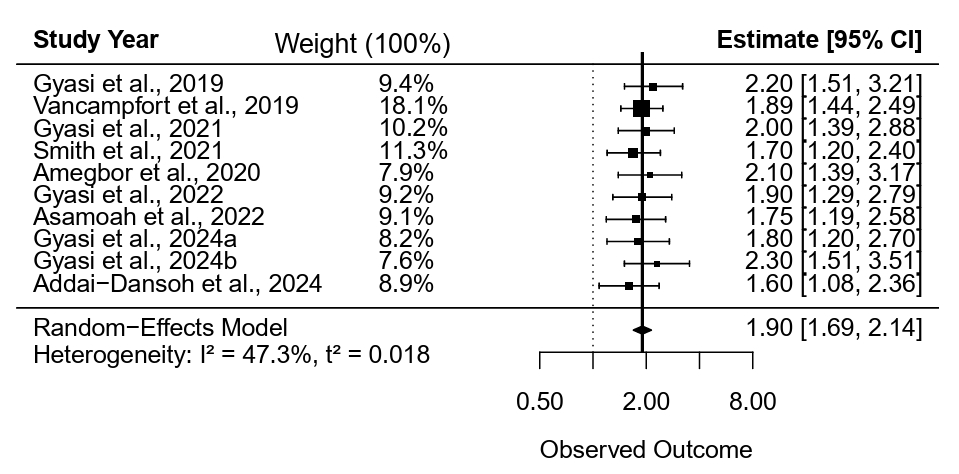
Effects of Socioeconomic Status (SES) Factors on Social Isolation/Loneliness (Meta-Analysis).
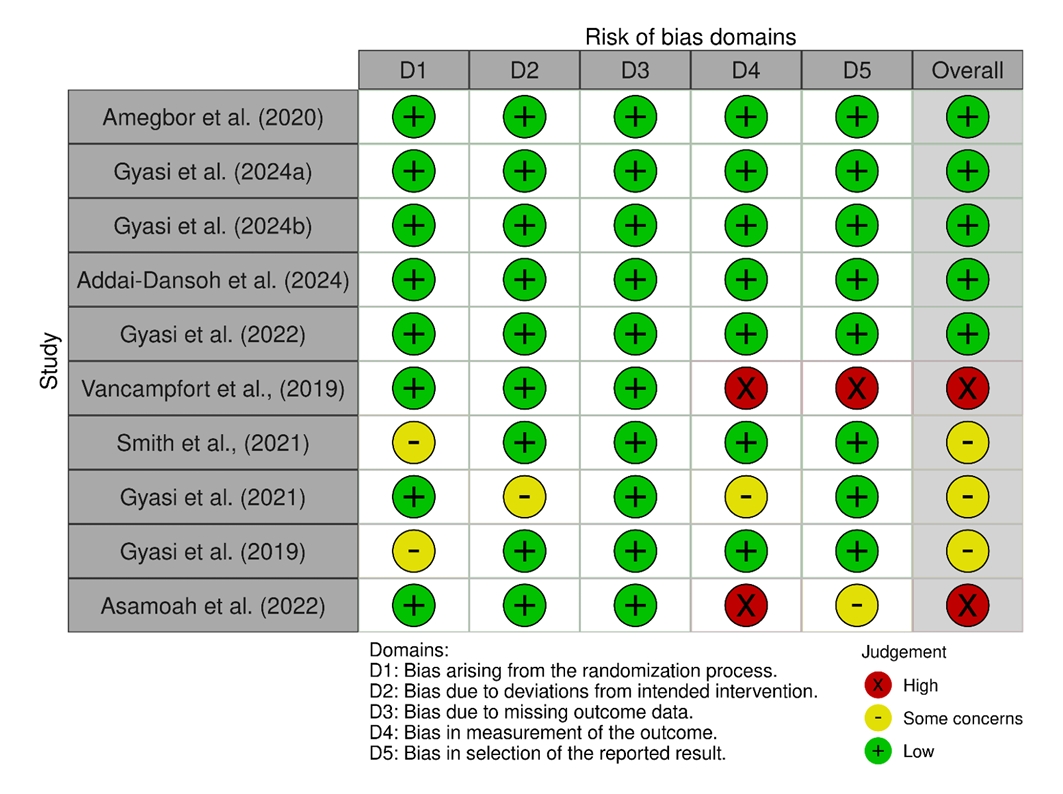
Risk of Bias Assessment for Included Studies (ROB2 domains).
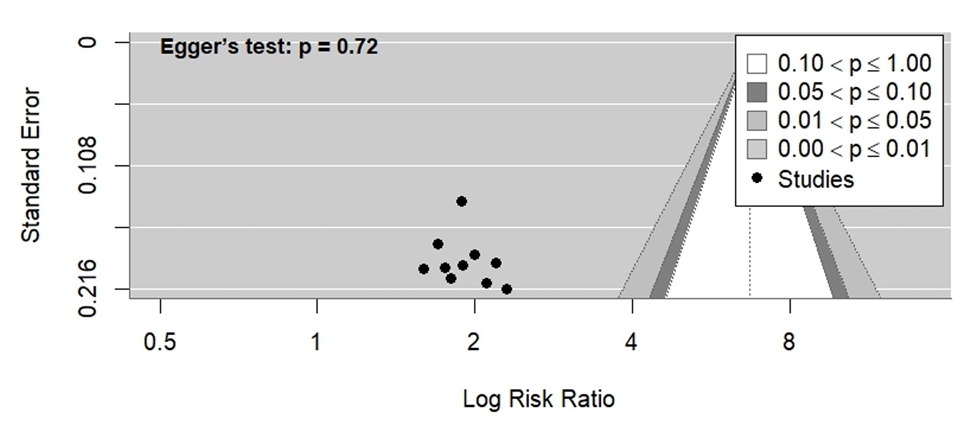
Funnel Plot with Egger’s Test for Social Isolation/loneliness Studies.
Study-Level Observations
Key findings from Table 1 reveal a pattern of elevated risk for social isolation and loneliness linked to adverse socioeconomic conditions. Across the studies, low socioeconomic conditions are characterised by factors such as area-level deprivation, low wealth, poverty, low education, food insecurity, and rural residency, which consistently predicted higher odds of isolation or loneliness. For instance, Gyasi et al. (2019) reported an odds ratio (OR) of 2.2 (95% CI: 1.5–3.2) for isolation in deprived neighbourhoods, highlighting rural poverty as a critical driver. Similarly, Amegbor et al. (2021) found an OR of 2.1 (95% CI: 1.4–3.2) associating low income and rural residence with social frailty, a construct overlapping with isolation. Food insecurity emerged as a particularly strong correlate, with Gyasi et al. (2024a) indicating it was associated with up to 35% of the association between SES and isolation (OR = 1.8, 95% CI: 1.2–2.7) and Asamoah et al. (2022) linking it to poor sleep via isolation (OR = 1.75, 95% CI: 1.2–2.6). Given the cross-sectional design of all studies, these associations suggest potential pathways but do not establish causality (Hajek et al., 2023). Gender and age interactions were noted in some studies, such as Gyasi et al. (2024b), where low SES amplified loneliness in women (OR = 2.3, 95% CI: 1.5–3.5). Protective factors included higher education and employment, which reduced isolation by up to 25% (Addai-Dansoh et al., 2024; OR = 1.6, 95% CI: 1.1–2.4), and urban residency, which buffered against rural-urban disparities.
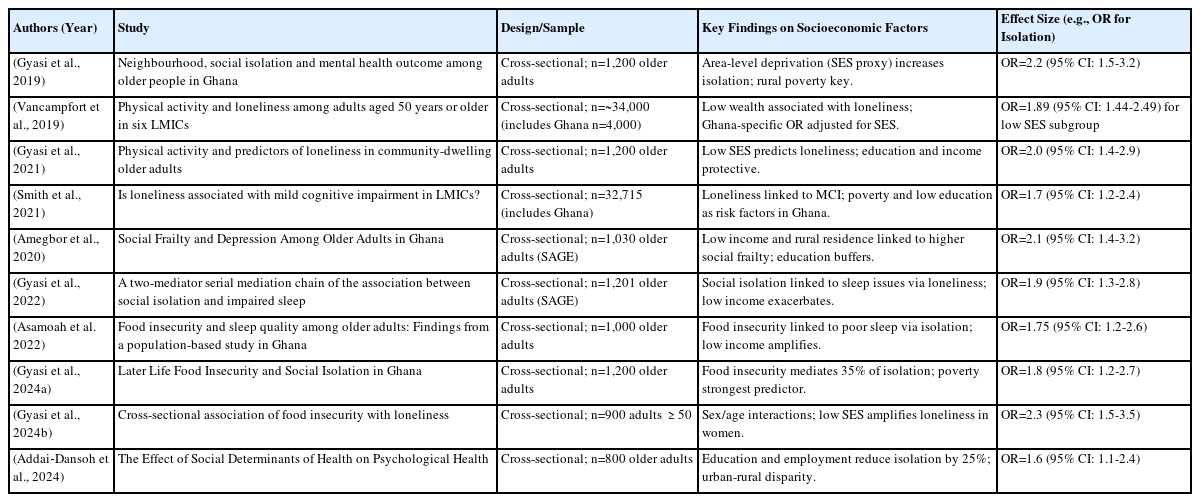
Characteristics of Included Studies Evaluating Social Isolation (2019—2024)
Weights vary from 7.6% (Gyasi et al., 2024b) to 18.1% (Vancampfort et al., 2019), reflecting greater influence from studies with narrower CIs (higher precision). No-table higher-weighted studies included Vancampfort et al. (2019; 18.1%) and Smith et al. (2021; 11.3%), likely due to larger samples or tighter estimates.
Overall, the results interpret low SES as a multifaceted risk factor that exacerbates social disconnection through material deprivation, limited access to resources, and environmental constraints in Ghana's aging population.
4. Discussion and Conclusions
Discussion
The results reveal a complex interaction between socioeconomic disadvantage and social isolation/loneliness in Ghana, a lower-middle-income country (LMIC) experiencing rapid demographic aging alongside enduring inequalities. The con-sistent odds ratios (ORs) observed across studies, averaging at 1.9, suggest that older adults in low-socioeconomic status (SES) groups are nearly twice as likely to expe-rience isolation, which can exacerbate health issues such as declines in mental health, mild cognitive impairment, and sleep disturbances (Gyasi et al., 2022; Asamoah et al., 2022). This finding is consistent with global data from LMICs, where significant socioeconomic disparities are prevalent due to insufficient social safety nets and pressures from urbanization (Stickley et al., 2020).
In Ghana, rural-urban divides contribute to elevated isolation risks for rural dwellers (Amegbor et al., 2021; Addai-Dansoh et al., 2024) with the effect of structural issues like limited infrastructure and migration patterns that erode traditional family support systems. Food insecurity, a proxy for extreme poverty, emerges as a pivotal cor-relate, associated with up to 35% of isolation effects in cross-sectional analyses (Gyasi et al., 2024a), which resonates with broader literature linking nutritional vulnerability to psychosocial stressors in aging populations (Gundersen & Ziliak, 2015). A recent population-based evidence further highlights the scale among Ghanaian older adults (aged ≥50), social isolation prevalence reaches 27.3% and loneliness 17.7%, with both independently linked to higher odds of probable de-pression (loneliness OR = 3.15, 95% CI 3.26–5.28; isolation OR = 1.24, 95% CI 1.10–1.41), and the loneliness-depression association amplified in rural areas (OR = 7.06 vs. 3.43 urban) (Gyasi et al., 2025).
Theoretically, these results support the convoy model of social relations (Kahn & Antonucci, 1980), suggesting that SES shapes the availability and quality of social networks over the life course. Low income and education may restrict opportuni-ties for social engagement, such as community activities or physical mobility, leading to loneliness and health declines (Gyasi et al., 2022). However, in Ghana’s context, this model may be extended to include cultural buffers such as inter-generational co-residence or community-based religious supports, which could moderate SES effects differently (Gyasi et al., 2023). For example, our findings suggest that rural-urban migration erodes these convoys more severely in low-SES groups, potentially explaining the heightened ORs compared to global estimates. Future studies could test competing mechanisms like whether limited digital connectivity in Ghana amplifies isolation beyond traditional factors, generating insight for sub-Saharan Africa’s unique aging trajectories (Adedeji et al., 2023; United Nations, 2020).
Gender-specific amplifications (Gyasi et al., 2024bf) suggest intersectional vul-nerabilities, where women in low-SES contexts face compounded risks from wid-owhood, caregiving burdens, and economic dependence areas warranting further disaggregated analyses. Comparatively, similar associations have been observed in high-income countries (United States-focused reviews; Courtin & Knapp, 2017). However, the magnitude in Ghana appears heightened (pooled OR = 1.90) compared to global estimates from high-income settings (typically ranging from 1.2 to 1.5 in meta-analyses; Ran et al., 2024; Chawla et al., 2021), likely due to weaker welfare systems, higher multidimensional poverty, and precarious aging circumstances in sub-Saharan Africa (Owusu-Addo et al., 2018). Compared to other LMICs like South Africa or India from SAGE data, Ghana’s rural-urban disparities may amplify SES effects, warranting cross-national analyses to iden-tify context specific moderators (Smith et al., 2021).
Key limitations include the reliance on cross-sectional designs, which prevents causal inferences and establishment of temporality. Reverse causation such as isolation perpetuating poverty through reduced productivity cannot be ruled out. The exclusion of qualitative studies and those with insufficient data for meta-analysis limits depth, particularly on lived experiences. Moreover, the focus on older adults overlooks younger cohorts, and the absence of longitudinal data hinders under-standing of trajectories. Heterogeneity in SES measurement (wealth quintiles vs. food insecurity scales) may introduce variability in the meta-analysis, though the PRIS-MA-compliant approach mitigates some biases.
Future research should prioritize prospective cohort studies to establish tempo-rality and explore interventions, such as SES-targeted programs like the livelihood empowerment program in Ghana, which could disrupt the isolation-poverty cycle (Owusu-Addo et al., 2018). Additionally, longitudinal designs could test Gha-na-specific moderators (kinship norms, migration effects, religious/community buffers, digital connectivity gaps) through comparative sub-Saharan African studies to generate novel theoretical insights for global aging research. Integrating mixed-methods approaches would enrich insights into cultural mediators.
Policymakers should leverage these findings to advocate for inclusive aging policies under frameworks like the UN Decade of Healthy Ageing (2021–2030), emphasizing equitable access to education, income support, and social infrastructure to foster resilience against isolation.
Conclusion
This review provides robust evidence that socioeconomic disadvantage is a sig-nificant and consistent predictor of social isolation and loneliness among older Ghanaian adults. Across the 10 included studies, low socioeconomic status mani-fested through poverty, low income, limited education, food insecurity, and rural residence was associated with substantially elevated odds of social isolation or loneliness, with effect sizes ranging from OR = 1.6 to 2.3 with a pooled effect 1.9. Food insecurity appeared as a particularly strong correlate, associated with up to 35% of the link between SES and isolation in key studies, while higher education and urban residence offered protective effects (Gyasi et al., 2024a; Addai-Dansoh et al., 2024).
These findings highlight the structural roots of social disconnection in Ghana’s older population, where material deprivation meets with weakening traditional support systems amid rapid socioeconomic and demographic transitions. Recent evidence underscores the urgency: prevalence of social isolation reaches 27.3% and lone-liness 17.7% among older adults in Ghana, with both independently linked to higher odds of probable depression (OR = 3.15 for loneliness; OR = 1.24 for isolation) and mediated by psychosocial factors like sleep problems and anxiety (Gyasi et al., 2025). Rural areas show amplified risks (loneliness-depression OR up to 7.06), reflecting migration patterns that erode intergenerational kinship networks and leave many older adults ageing in solitude or experiencing persis-tent loneliness (Conduah, 2025). Compared to global high-income and other LMICs, Ghana's associations appear heightened due to multidimensional poverty, limited welfare, and rapid urbanization (Ran et al., 2024; Chawla et al., 2021).
Social isolation and loneliness, in turn, are not merely individual experiences but outcomes of broader social determinants, with implications for mental health, cog-nitive function, sleep quality, and overall well-being in later life (Gyasi et al., 2022; Asamoah et al., 2022). The consistency of results, despite variations in SES meas-urement and sample characteristics, underscores the persistent influence of socio-economic inequalities on social health in this lower-middle-income context.
From a public health and policy perspective, these results call for targeted in-terventions that address upstream socioeconomic drivers rather than solely down-stream symptoms of isolation. Strengthening social protection programs such as expanding access to pensions, improving the current Livelihood Empowerment Against Poverty (LEAP) program, investing in agricultural for food security, and promoting education opportunities could mitigate risks, particularly for rural dwellers, women, and those experiencing multidimensional poverty. Community-based strategies should leverage Ghana's cultural strengths (religious and family net-works, potential for intergenerational engagement) while tackling emerging challenges like digital gaps. Interventions targeting psychosocial mediators such as sleep hygiene, depression screening and promoting social participation (age-friendly community activities) are promising, as recent studies show they can buffer isolation's health impacts (Oduro, 2024).
These recommendations align with the United Nations Sustainable Develop-ment Goals, particularly SDG 1 (No Poverty) and SDG 3 (Good Health and Wellbeing) and the UN Decade of Healthy Ageing (2021–2030), emphasizing eq-uitable access to resources and social infrastructure to foster resilience against disconnection.
In summary, reducing socioeconomic disparities is essential to preventing social isolation and loneliness among older Ghanaians. The evidence though cross-sectional, points to a clear pathway: upstream SES-focused policies can disrupt the deprivation and disconnection cycle. Future longitudinal and intervention research is needed to confirm causality and evaluate the effectiveness of SES-sensitive policies through comparative studies across sub-Saharan Africa and whether Ghana’s cultural support system uniquely moderate SES-isolation links, generating new theoretical insights for global aging research.
Notes
Data Availability
All data analyzed in this systematic review and meta-analysis were extracted from published studies. No new datasets were generated.
Code Availability
Analyses were conducted in R (metafor package). Example code for effect size harmonization, meta-analysis, and visualization is available from the first author upon reasonable request.
Author Contributions
P.A.A. designed the review and conducted the statistical analysis, screened the studies and drafted the manuscript. S.S.O. provided oversight, contributed to methodological framing, and revised the manuscript for policy and institutional relevance, public health interpretation and provided critical revisions. All authors approved the final version of the manuscript.
Conflicts of Interest
The authors declare no competing interests.