Articles
- Page Path
- HOME > IGEE Proc > Volume 3(1); 2026 > Article
-
Article
Individual and Socioeconomic Determinants of Antenatal Care Access for Disadvantaged Pregnant Women: A Systematic Review and Empirical Analysis - Rani Wulandari*
-
IGEE Proc 2026;3(1):38-46.
DOI: https://doi.org/10.69841/igee.2026.004
Published online: February 26, 2026
Department of Global Health Security, Yonsei University, Seoul, Korea
- *Corresponding author: Rani Wulandari, E-mail: wulandarirani@yonsei.ac.kr
• Received: January 9, 2026 • Revised: February 6, 2026 • Accepted: February 9, 2026
© 2026 by the authors.
Submitted for possible open-access publication under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
- 800 Views
- 22 Download
Abstract
- Socioeconomic disadvantage has consistently been associated with reduced maternal healthcare utilization; however, the extent to which individual-level socioeconomic and demographic characteristics explain antenatal care (ANC) access remains uncertain. This study examined associations between socioeconomic status (SES), basic demographic factors, and ANC completion, while synthesizing global evidence on social vulnerability and maternal healthcare access among disadvantaged pregnant women. The analysis combined secondary data from 2,019 women obtained from the Institute for Health Metrics and Evaluation (IHME) dataset with a systematic review and meta-analysis conducted in accordance with the PRISMA 2020 guidelines. Multivariable logistic regression and exploratory machine learning approaches (K-Nearest Neighbors and XGBoost) were applied to assess the discriminative capacity of individual-level variables for ANC completion. A random-effects me-ta-analysis was used to synthesize adjusted odds ratios (aORs) from eligible observational studies. In the IHME dataset, SES was not significantly associated with ANC completion after adjustment (aOR = 0.97; 95% CI: 0.78–1.21), and individual-level models demonstrated limited discriminatory performance (AUC range: 0.49–0.50). In contrast, the meta-analysis of six studies showed that socioeconomic disadvantage was significantly associated with inadequate or delayed prenatal care (pooled aOR = 1.96; 95% CI: 1.26–3.07), with substantial heterogeneity across studies. Although conceptually distinct, indicators such as migrant status and neighborhood risk were synthesized as proxies of broader social vulnerability. Overall, these findings suggest that individual-level so-cioeconomic and demographic variables alone provide limited explanatory value for maternal healthcare utilization, highlighting the potential importance of broader structural and health system-level factors influencing access to antenatal care.
- Access to routine maternal healthcare is strongly shaped by socioeconomic conditions, with disadvantaged populations consistently experiencing greater barriers to timely and adequate care. Previous studies have shown that pregnant women from lower socioeconomic status (SES) backgrounds face compounded challenges, including financial constraints, limited transportation options, and reduced access to social support networks, all of which may hinder engagement with antenatal care (ANC) services (Oh et al., 2021; Bellerose et al., 2022).
- Beyond material deprivation, socioeconomic disadvantage is frequently associated with forms of social vulnerability that constrain access to both formal healthcare systems and informal support mechanisms. Financial insecurity may necessitate prioritization of basic needs such as food and housing, leaving limited capacity to sustain communication resources or engage with community-based services. In parallel, geographic and infrastructural barriers, including limited transportation availability, can restrict mobility and reduce opportunities for social connectedness, further complicating access to maternal healthcare.
- These intersecting constraints contribute to conditions of social vulnerability, in which pregnant women may experience reduced informational, emotional, and logistical support. Understanding how such vulnerabilities relate to maternal healthcare utilization is critical for identifying populations at risk of inadequate ANC engagement. However, existing evidence has largely focused on establishing associations between socioeconomic disadvantage and maternal health outcomes, with less attention to the extent to which individual-level socioeconomic and demographic characteristics can account for observed differences in care utilization.
- Moreover, while socioeconomic disadvantage is widely recognized as a determinant of maternal healthcare access, findings across settings remain heterogeneous, reflecting variations in health system organization, social protection mechanisms, and population characteristics. This heterogeneity complicates efforts to generalize individual-level determinants across contexts and underscores the need for evidence synthesis alongside empirical analysis of individual-level data.
- Therefore, this study aimed to address two complementary objectives: (1) to examine associations between socioeconomic status, basic demographic characteristics, and ANC completion using multivariable regression and exploratory modeling approaches applied to secondary survey data; and (2) to synthesize global evidence on socioeconomic disadvantage and social vulnerability in relation to maternal healthcare access through a systematic review and meta-analysis. By integrating individual-level analysis with systematic evidence synthesis, this study seeks to clarify the explanatory scope and limitations of individual-level determinants in understanding disparities in antenatal care access.
1. Introduction
- Material
- This study utilized two primary data sources. First, secondary individual-level data were obtained from a global maternal health survey administered via the Premise platform and released on September 14, 2021, by the Institute for Health Metrics and Evaluation (IHME). The dataset contains standardized information on antenatal care utilization and selected demographic characteristics among pregnant women and recent mothers across multiple countries.
- Second, evidence from published observational studies was identified and synthesized through a systematic review conducted in accordance with the PRISMA 2020 guidelines. Reference management and screening procedures were supported using Mendeley Reference Manager. All statistical analyses and evidence synthesis were performed using R statistical software (version 4.3.1).
- Methods
- Participants: For the secondary data analysis, the study included a global sample of 2,282 respondents from 51 countries. Data were collected between May and June 2021 using a smartphone-based survey platform. Eligible respondents were women who were currently pregnant or had given birth within the preceding six months at the time of data collection. Although the sampling strategy employed target quotas and does not yield a nationally representative sample, the dataset provides cross-sectional individual-level information relevant to maternal healthcare utilization across diverse settings.
- For the systematic review, eligible studies comprised observational research in-volving pregnant women from socioeconomically disadvantaged populations and reporting outcomes related to antenatal care utilization, access to maternal healthcare services, or related measures of social vulnerability. Studies were required to report adjusted effect estimates to be included in the quantitative synthesis.
2. Materials and Methods
- This section presents findings from the secondary individual-level data analysis, followed by classification model performance and the synthesis of evidence from the systematic review and meta-analysis. Results are reported sequentially from descriptive analyses to multivariable modeling and quantitative evidence synthesis.
- Primary Data Analysis: Determinants and Predictive Modeling of ANC Completion (IHME Dataset)
- Descriptive and Bivariate Analysis (IHME Dataset)
- Among the 2,019 women included in the analysis, antenatal care (ANC) completion rates were similar across socioeconomic groups. The ANC completion rate was 80.0% among women in the high/middle socioeconomic status (SES) group and 79.6% among those in the low SES group (Table 1).
- Chi-square analysis indicated no statistically significant association between SES and ANC completion (p = 0.851). Bivariate analyses further showed no significant associations between ANC completion and maternal age group or geographic indicators where available (Table 2).
- Multivariate Logistic Regression
- Multivariable logistic regression analysis did not identify statistically significant associations between individual-level demographic characteristics and ANC completion (Table 3). After adjustment, women in the low SES group had similar odds of ANC completion compared with those in the high/middle SES group (adjusted OR = 0.97; 95% CI: 0.78–1.21; p = 0.785). Maternal age group was likewise not significantly associated with ANC completion. Variance Inflation Factor (VIF) values for all predictors were below 2, indicating no evidence of multicollinearity.
- K-Nearest Neighbors (KNN) Classification
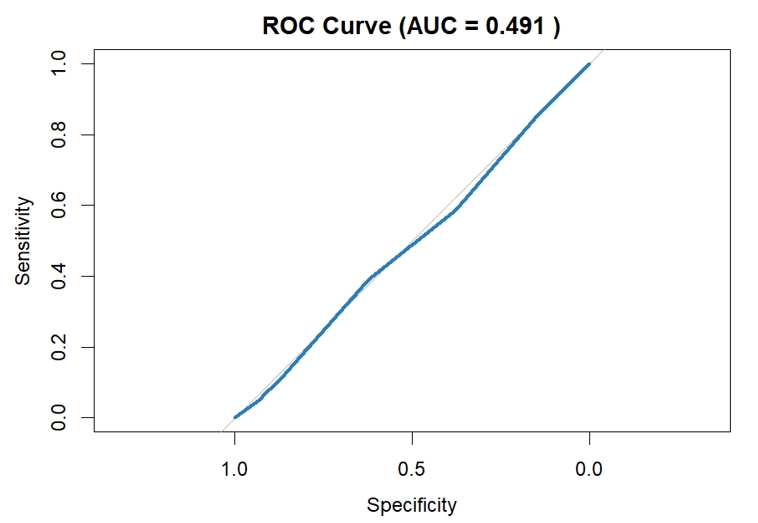
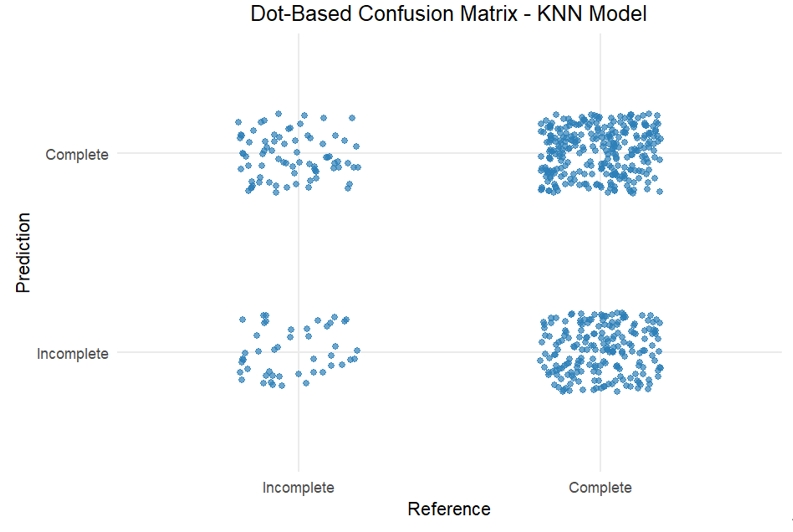
- A K-Nearest Neighbors (KNN) classification model was applied to distinguish be-tween completed and incomplete ANC visits using SES and maternal age group as predictors. Class imbalance was addressed through up-sampling during 10-fold cross-validation. The optimized KNN model (k = 15) achieved an accuracy of 54.4% and an area under the receiver operating characteristic curve (AUC) of 0.491, indicating limited discriminative capacity. Sensitivity for identifying completed ANC visits was 58.6%, while specificity for identifying incomplete ANC visits was 37.7% (Table 4). The ROC curve approximated the diagonal line, and the confusion matrix showed substantial misclassification of incomplete ANC visits (Figures 1 and 2).
- Boosting (XGBoost) Classification
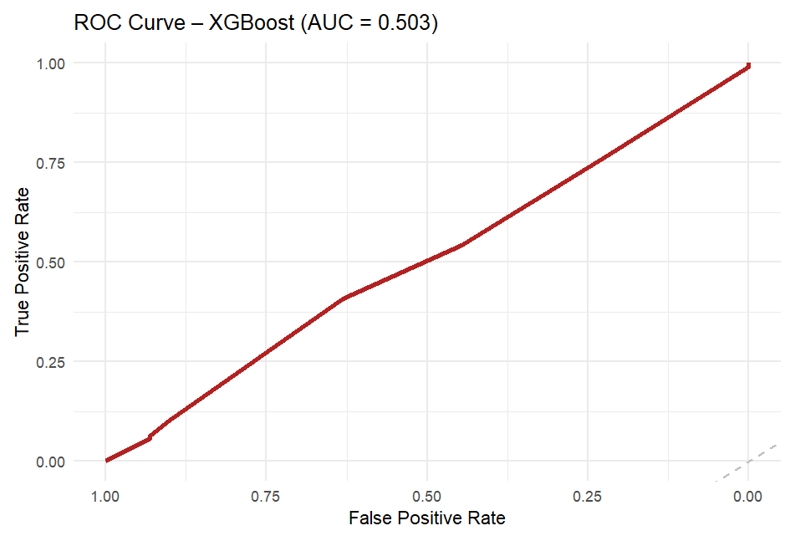
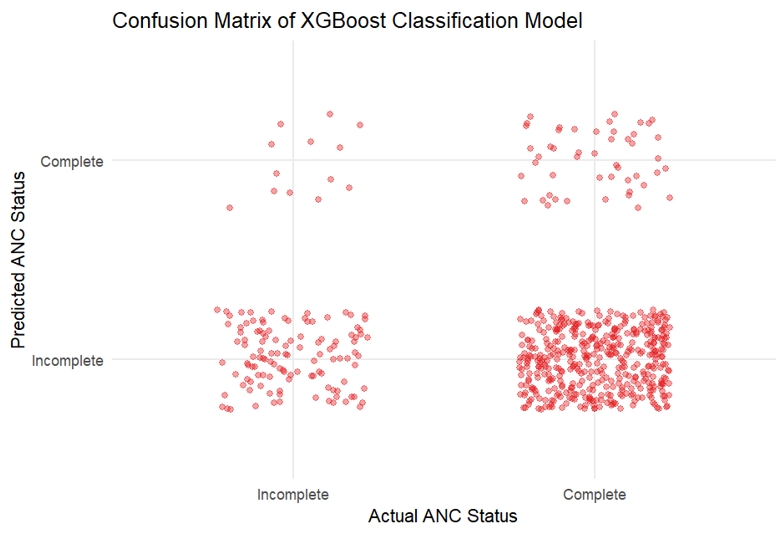
- The gradient boosting model yielded an AUC of 0.503, indicating no meaningful improvement in classification performance relative to chance. The confusion matrix demonstrated high specificity (90.0%) but low sensitivity (10.3%), reflecting pre-dominant classification into the majority outcome category (Table 5; Figures 3 and 4). The low overall accuracy observed in this model is attributable to the use of aggressive up-sampling strategies to address class imbalance, which altered class distributions during model training and evaluation and prioritized sensitivity to minority outcomes over raw classification accuracy.
- Meta-Analysis of Global Evidence
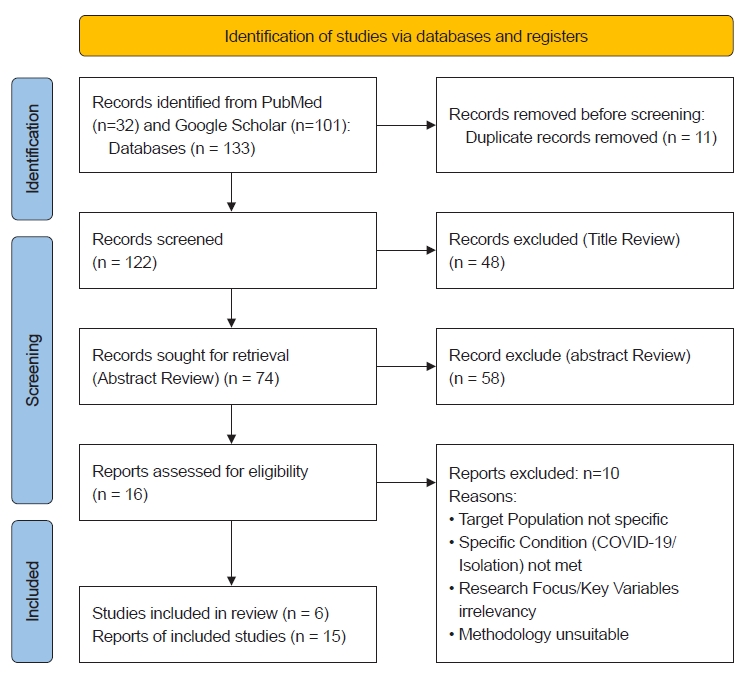
- The systematic literature search identified 133 records. After removal of duplicates and screening procedures, six studies met the eligibility criteria and were included in the final quantitative synthesis (Figure 5). The characteristics of the included studies are summarized in Table 6.
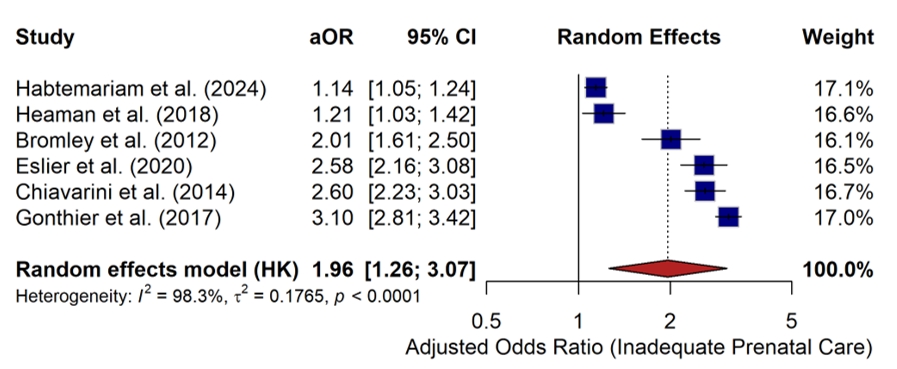
- A random-effects meta-analysis was conducted using adjusted odds ratios (aORs) from the six included studies to examine the association between socioeconomic disadvantage and antenatal care utilization. The pooled analysis showed that socio-economic disadvantage was associated with a higher likelihood of inadequate or delayed antenatal care (pooled aOR = 1.96; 95% CI: 1.26–3.07; p < 0.001) (Figure 6). Study-specific adjusted odds ratios from the included studies are presented in Table 7. Substantial heterogeneity was observed across studies (I² = 98.3%; p < 0.0001), reflecting differences in study populations, exposure definitions, and healthcare system contexts.
- The included studies were conducted in diverse geographic settings, including Europe and North America, and employed heterogeneous indicators of socioeconomic disadvantage, such as area-level deprivation indices, migrant status, ethnicity, neighborhood risk, and social isolation. Although these exposures represent conceptually distinct constructs, they were synthesized as proxy indicators of broader socioeconomic vulnerability for the purpose of quantitative pooling. Across all included studies, the direction of association between socioeconomic disadvantage and inadequate antenatal care was consistent, despite considerable variability in effect size magnitude.
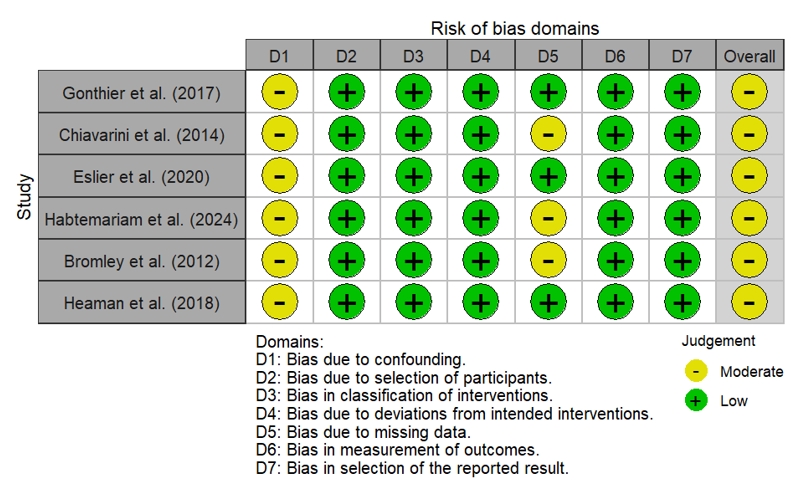
- Differences in effect estimates were influenced by study design and population size. Large population-based studies, such as Habtemariam et al. (2024) and Heaman et al. (2018), reported more modest associations (aORs of 1.14 and 1.21, respectively), whereas smaller European cohort studies, including Gonthier et al. (2017), observed larger effect sizes (aOR = 3.10). This variability underscores the heterogeneity of contexts and measurement approaches across studies included in the synthesis. Overall risk of bias across the included studies was assessed using the ROBINS-I tool (Figure 7).
3. Results
- This study examined the extent to which individual-level socioeconomic and demographic characteristics are associated with maternal healthcare utilization, while synthesizing global evidence on socioeconomic disadvantage and related forms of social vulnerability. The findings demonstrate a clear contrast between individual-level analyses and population-level evidence. While the meta-analysis identified a consistent association between socioeconomic disadvantage and inadequate ante-natal care across diverse settings, the analysis of the IHME dataset showed that basic demographic characteristics alone provided limited explanatory value for antenatal care (ANC) completion.
- Multivariable regression analyses did not identify significant associations between individual demographic predictors and ANC completion, and exploratory classification models demonstrated limited discriminative capacity. These results suggest that, within the constraints of the available individual-level data, maternal healthcare utilization cannot be adequately explained by age or socioeconomic status alone. Rather than indicating the absence of socioeconomic influence, these findings highlight the limited ability of individual-level demographic variables to capture the complexity of healthcare access pathways.
- The meta-analysis provides complementary context by demonstrating that indicators of socioeconomic disadvantage including area-level deprivation, migrant status, ethnicity, neighborhood risk, and social isolation are associated with inadequate antenatal care across multiple healthcare systems. Although these indicators represent conceptually distinct constructs, their consistent direction of association suggests that broader forms of social vulnerability are relevant to maternal healthcare utilization at the population level. Although operationalized differently, these indicators converge in representing systemic barriers to healthcare access, such as institutional exclusion, geographic marginalization, and limited social support. However, the substantial heterogeneity observed across studies underscores the importance of contextual factors, including differences in health system organization, social protection mechanisms, and measurement approaches. The extremely high heterogeneity likely reflects substantial differences in the operationalization of socioeconomic vulnerability across studies, such as individual migrant status in France, ethnicity-based classification in the United States, and area-level deprivation indices in population-based cohorts. These definitional inconsistencies highlight the absence of standardized measures for social vulnerability in maternal health research.
- Importantly, the contrast between the weak explanatory performance of individual-level models and the stronger associations observed in population-based studies suggests that unmeasured structural and system-level factors may play a role in shaping access to maternal healthcare. Such factors may include healthcare availability, transportation barriers, indirect costs, and institutional accessibility, none of which were directly captured in the individual-level dataset used in this study. These interpretations should therefore be understood as plausible explanations rather than causal conclusions.
- Several limitations should be acknowledged. The secondary data analysis relied on a limited set of individual-level demographic variables, which constrained the scope of explanatory modeling. Structural determinants were not directly measured, and residual confounding cannot be excluded. In addition, the meta-analysis incorporated studies conducted across different time periods and healthcare contexts, contributing to substantial heterogeneity. Despite these limitations, the integration of individual-level analysis with systematic evidence synthesis provides a nuanced perspective on the strengths and limitations of demographic predictors in understanding maternal healthcare utilization.
4. Discussion
- This study demonstrates that individual-level demographic characteristics alone provide limited explanatory value for antenatal and postnatal care completion. Analyses using multivariable regression and exploratory modeling approaches showed that age and basic socioeconomic indicators were insufficient to distinguish between completed and incomplete maternal healthcare utilization within the available individual-level data.
- At the same time, the synthesis of global evidence indicates that socioeconomic disadvantage is consistently associated with inadequate antenatal care across diverse settings. Taken together, these findings suggest that disparities in maternal healthcare utilization cannot be fully understood through individual-level characteristics alone and may be shaped by broader social and health system contexts.
- Future research should prioritize the integration of system-level and structural variables, including healthcare accessibility, transportation constraints, and indirect costs, to more comprehensively capture the determinants of maternal healthcare access and better bridge individual-level analyses with population-level evidence.
- From a policy perspective, these findings underscore the need for maternal health interventions that extend beyond individual-level education and address structural barriers such as transportation access, institutional navigation, and service availability.
5. Conclusions
Figure 1.Receiver Operating Characteristic (ROC) Curve of the KNN Model for ANC Completion (AUC = 0.491).
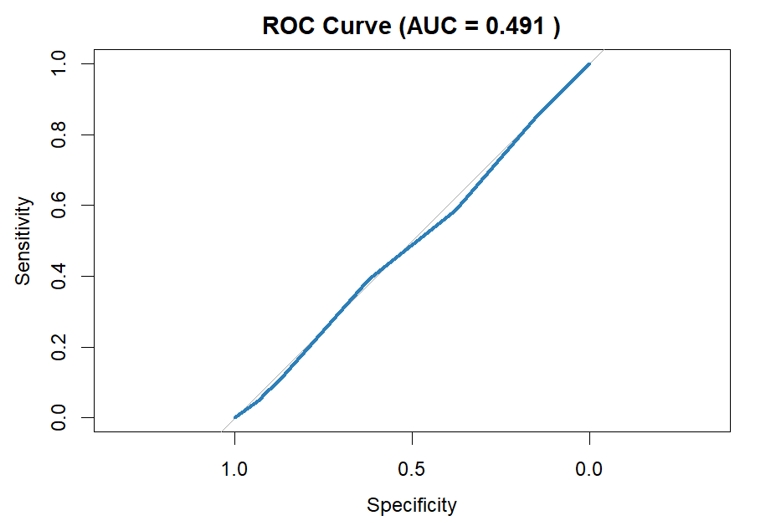
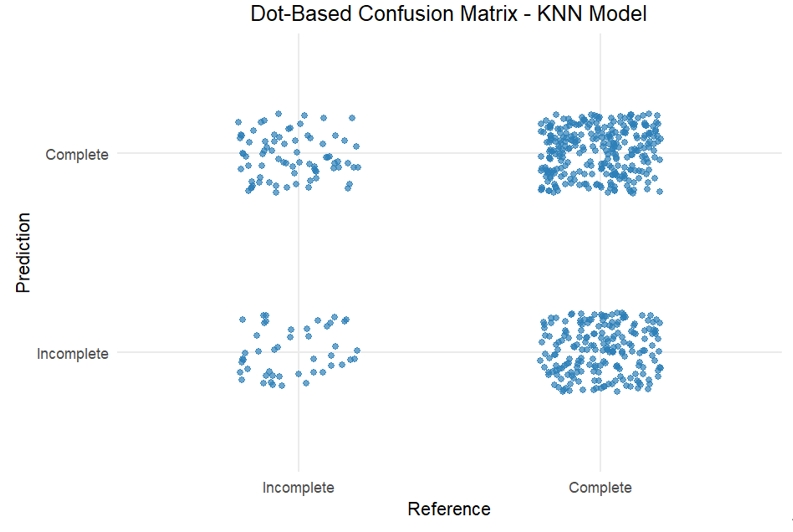
Figure 3.Receiver Operating Characteristic (ROC) Curve of the XGBoost Model for ANC Completion (AUC = 0.503).
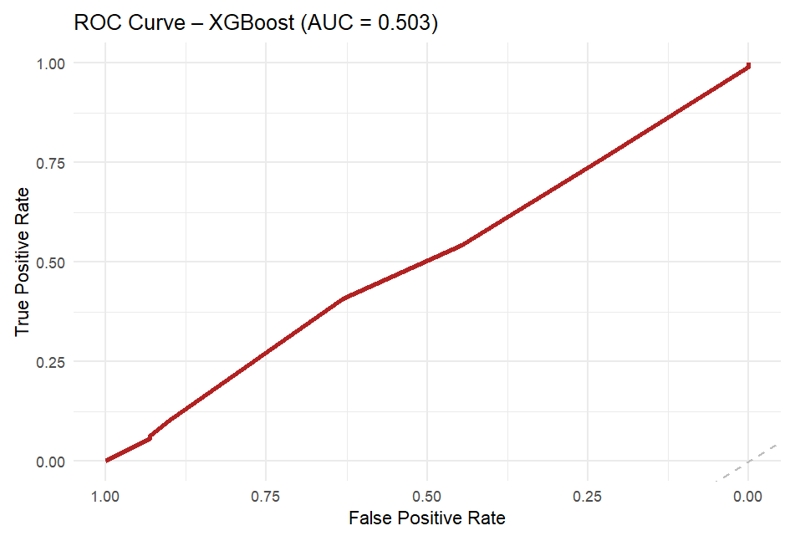
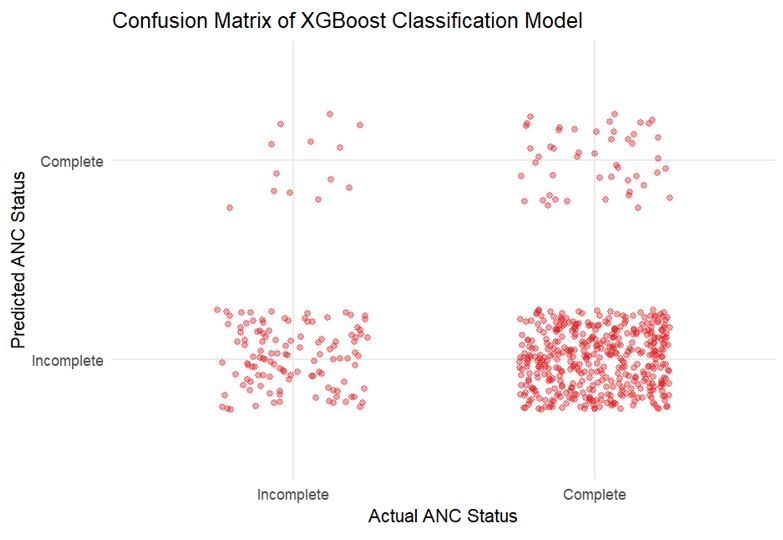
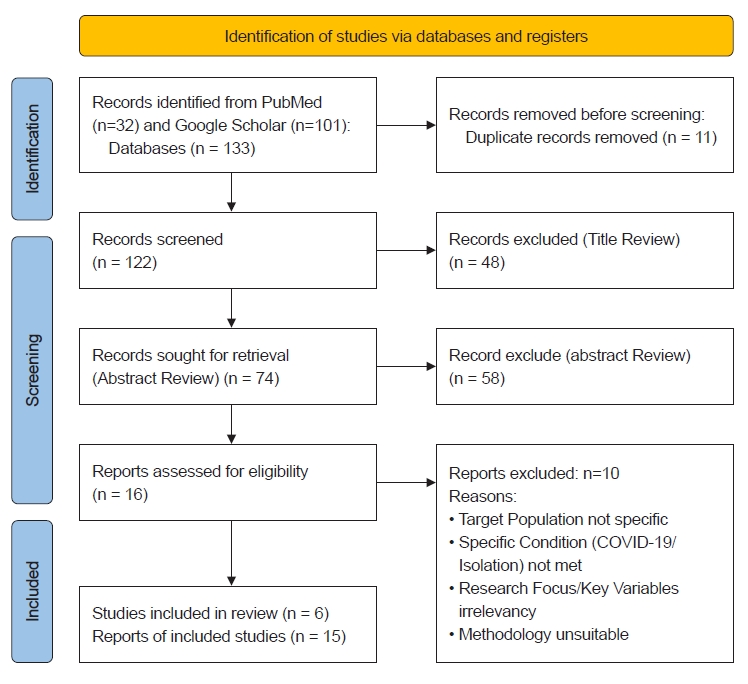
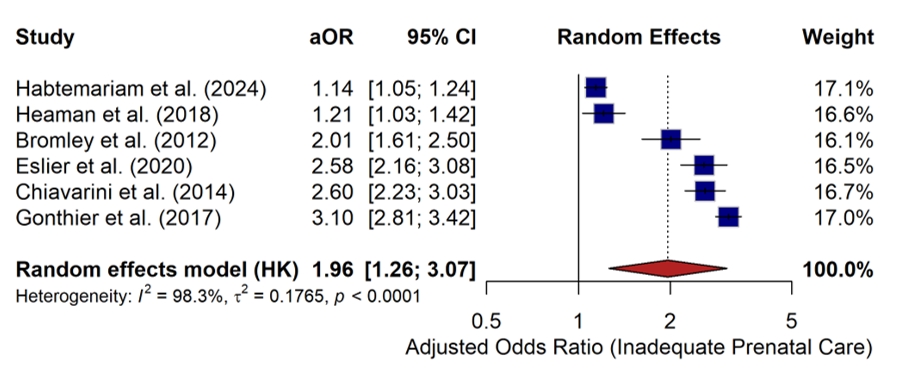
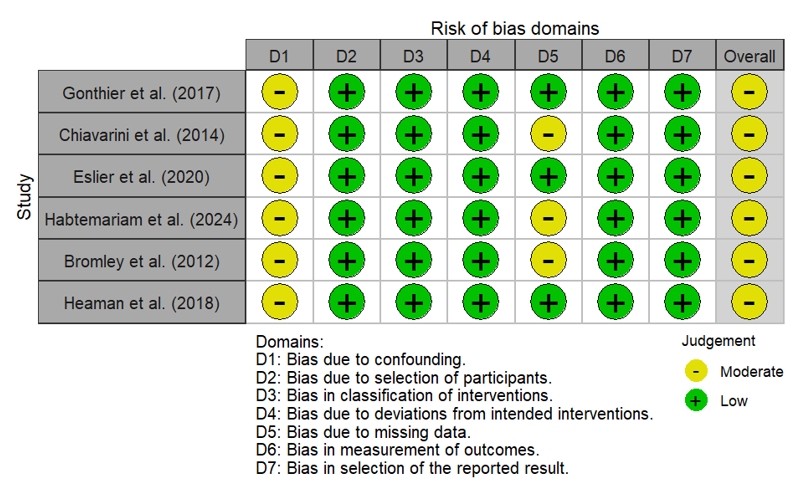
Table 1.ANC Completion by Socioeconomic Status
| SES | ANC Incomplete (n) | ANC Complete (n) | Total | Completion Rate (%) |
|---|---|---|---|---|
| High/Middle SES | 211 | 844 | 1055 | 80.0 |
| Low SES | 197 | 767 | 964 | 79.6 |
Table 2.Bivariate associations between demographic factors and ANC/PNC completion
| Variable | p-value |
|---|---|
| SES vs ANC | 0.851 |
| Age group vs ANC | 0.708 |
| Geography vs PNC | 0.964 |
Table 3.Multivariate Logistic Regression Analysis of Factors Associated with ANC Completion
| Predictor | Adjusted OR (95% CI) | p-value |
|---|---|---|
| Low SES | 0.97 (0.78–1.21) | 0.785 |
| Age 16–25 | 0.89 (0.33–2.04) | 0.798 |
| Age 26–35 | 0.83 (0.31–1.91) | 0.683 |
Table 4.Performance Metrics of the KNN Classification Model
Table 5.Performance Metrics of the XGBoost Classification Model
| Metric | Value |
|---|---|
| Accuracy | 0.274 |
| Sensitivity | 0.103 |
| Specificity | 0.900 |
Table 6.Characteristics of Included Studies Examining Socioeconomic Disadvantage and Antenatal Care Utilization
| No | Author (Year) | Country / Region | Study Design | Data Source & Sample Size | Exposure (Social/Structural Disadvantage) | Outcome | Effect Size (Adjusted) |
|---|---|---|---|---|---|---|---|
| 1 | Gonthier et al. (2017) | France | Secondary analysis of a prospective cohort | PreCARE cohort; N = 9,770 | High Social Deprivation (synthetic index) | Inadequate prenatal care utilization | 3.10 (2.80 – 3.40) |
| 2 | Chiavarini et al. (2014) | Italy (Umbria) | Retrospective population-based study | Administrative births certificate (SCLB) (N ≈ 37.000) | Foreign-born status (Extra EU-27) | Late initiation and inadequate prenatal care | 2.60 (2.25 – 3.05) |
| 3 | Eslier et al. (2020) | France | Prospective cohort | PreCARE prospective cohort; N = 9.599 | Undocumented migrant status | Inadequate prenatal care utilization | 2.58 (2.16 – 3.07) |
| 4 | Habtemariam et al. (2024) | USA (Rhode Island) | Population-based retrospective cohort | Vital Statistics birth certificates (2005-2014); N=97.249 | High neighborhood risk (socioeconomic index) | Less than adequate prenatal care | 1.14 (1.05 – 1.24) |
| 5 | Bromley et al. (2012) | USA (Rhode Island) | Retrospective cohort study | RI PRAMS surveillance data; N = 9,906 | Hispanic ethnicity (vs Non-Hispanic White) | Delayed and inadequate prenatal care | 2.01 (1.61 – 2.50) |
| 6 | Heaman et al. (2018) | Canada (Manitoba) | Population-based retrospective cohort | Administrative databases (N ≈ 68,132) | Social Isolation | Inadequate prenatal care utilization | 1.21 (1.03 – 1.42) |
Table 7.Summary of Adjusted Odds Ratios (aOR) for the Association Between Socioeconomic Disadvantage and Inadequate Prenatal Care
| No | Study | Country | Exposure | Outcome | aOR (95% CI) |
|---|---|---|---|---|---|
| 1 | Gonthier et al. (2017) | France | High Social Deprivation (Q4 vs Q1) | Inadequate Care | 3.10 (2.80 – 3.40) |
| 2 | Chiavarini et al. (2014) | Italy | Deprivation Index (High vs Low) | Late/Inadequate Care | 2.60 (2.25 – 3.05) |
| 3 | Eslier et al. (2020) | France | Undocumented Migrant Status | Inadequate Care | 2.58 (2.16 – 3.07) |
| 4 | Habtemariam et al. (2024) | USA | High Neighborhood Risk | Inadequate Care | 1.14 (1.05 – 1.24) |
| 5 | Bromley et al. (2012) | USA | Hispanic (vs Non-Hispanic White) | Delayed/Inadequate | 2.01 (1.61 – 2.50) |
| 6 | Heaman et al. (2018) | Canada | Social Isolation | Inadequate Care | 1.21 (1.03 – 1.42) |
- Azria, E. (2015). Inequality in prenatal care use. The Lancet, 385(9976), 1401. https://doi.org/10.1016/S0140-6736(15)60714-XArticle
- Bellerose, M., Rodriguez, M., & Vivier, P. M. (2022). A systematic review of the qualitative literature on barriers to high-quality prenatal and postpartum care among low-income women. Health Services Research, 57(4), 775-785. https://doi.org/10.1111/1475-6773.14008ArticlePubMedPMC
- Bromley, E., Nunes, A., & Phipps, M. G. (2012). Disparities in pregnancy healthcare utilization between Hispanic and non-Hispanic White women in Rhode Island. Maternal and Child Health Journal, 16(8), 1576-1582. https://doi.org/10.1007/s10995-011-0850-5ArticlePubMed
- Bustani, M. (2023). Digital health equity in maternal care: A scoping review. Frontiers in Public Health, 11, Article 11523. https://doi.org/10.3389/fpubh.2023.11523Article
- Chiavarini, M., Lanari, D., Minelli, L., & Salmasi, L. (2014). Socio-demographic determinants and access to prenatal care in Italy. BMC Health Services Research, 14(1), Article 174. https://doi.org/10.1186/1472-6963-14-174ArticlePubMedPMC
- Chmielewska, B., Barratt, I., Townsend, R., Kalafat, E., van der Meulen, J., Gurol-Urganci, I., & Khalil, A. (2021). Effects of the COVID-19 pandemic on maternal and perinatal outcomes: A systematic review and meta-analysis. The Lancet Global Health, 9(6), e759-e772. https://doi.org/10.1016/S2214-109X(21)00079-6ArticlePubMedPMC
- Deneux-Tharaux, C. (2018). The PreCARE cohort: A multicenter prospective study of social deprivation and pregnancy. Paediatric and Perinatal Epidemiology, 32(1), 12-22. https://doi.org/10.1111/ppe.12417ArticlePubMedPMC
- El-Khoury Lesueur, F. (2018). The impact of migration and legal status on prenatal care and birth outcomes: The PreCARE cohort. Annals of Epidemiology, 28(10), 712-720. https://doi.org/10.1016/j.annepidem.2018.07.003Article
- Eslier, M., Deneux-Tharaux, C., Sauvegrain, P., Schmitz, T., Luton, D., Mandelbrot, L., Estellat, C., & Azria, E. (2020). Association between migrant women’s legal status and prenatal care utilization in the PreCARE cohort. International Journal of Environmental Research and Public Health, 17(10), Article 3462. https://doi.org/10.3390/ijerph17103462ArticlePubMedPMC
- Gonthier, C., Estellat, C., Deneux-Tharaux, C., Blondel, B., Alfaiate, T., Schmitz, T., & Azria, E. (2017). Association between maternal social deprivation and prenatal care utilization: The PreCARE cohort study. BMC Pregnancy and Childbirth, 17(1), Article 126. https://doi.org/10.1186/s12884-017-1310-zArticlePubMedPMC
- Habtemariam, H., Schlichting, L. E., Kole-White, M. B., Berger, B., & Vivier, P. (2024). Neighborhood risk and prenatal care utilization in Rhode Island, 2005–2014. Birth, 51(3), 560-571. https://doi.org/10.1111/birt.12810Article
- Heaman, M. I. (2015). Perceptions of barriers to prenatal care in inner-city Winnipeg. SAGE Open Medicine, 3, Article 2050312115621314. https://doi.org/10.1177/2050312115621314ArticlePubMedPMC
- Heaman, M. I., Martens, P. J., Brownell, M. D., Chartier, M. J., Thiessen, K. R., & Helewa, M. E. (2018). Inequities in utilization of prenatal care: A population-based study in the Canadian province of Manitoba. BMC Pregnancy and Childbirth, 18(1), Article 430. https://doi.org/10.1186/s12884-018-2061-1ArticlePubMedPMC
- Higgins, J. P. T., & Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21(11), 1539-1558. https://doi.org/10.1002/sim.1186ArticlePubMedPMC
- Khalil, A. (2020). Change in the incidence of stillbirth and preterm delivery during the COVID-19 pandemic. JAMA, 324(14), 1405-1406. https://doi.org/10.1001/jama.2020.12746ArticlePubMedPMC
- Kotelchuck, M. (1994). An evaluation of the Kessner Adequacy of Prenatal Care Utilization Index. American Journal of Public Health, 84(9), 1414-1420. https://doi.org/10.2105/AJPH.84.9.1414ArticlePubMedPMC
- Luo, Y. (2021). Telemedicine for antenatal care during COVID-19: A systematic review. International Journal of Gynecology & Obstetrics, 154(1), 1-9. https://doi.org/10.1002/ijgo.13547ArticlePubMed
- Madhi, S. A. (2022). Maternal health and COVID-19: A global perspective on risk and resilience. Vaccine, 40, 123-134. https://doi.org/10.1016/j.vaccine.2021.11.019ArticlePubMed
- Maldonado, L., & Read, J. G. (2015). Disparities in pregnancy healthcare utilization: The role of Hispanic ethnicity and acculturation. Ethnicity & Health, 20(4), 321-339. https://doi.org/10.1080/13557858.2014.907427Article
- Nunes, A. (2020). Socioeconomic status and birth outcomes: A 10-year review of Rhode Island data. Public Health Reports, 135(2), 234-245. https://doi.org/10.1177/0033354920904152Article
- Oh, S. S., Kim, K. A., Kim, M., Oh, J., Chu, S. H., & Choi, J. (2021). Measurement of digital literacy among older adults: A systematic review. Journal of Medical Internet Research, 23(2), e26145. https://doi.org/10.2196/26145ArticlePubMedPMC
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., & Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71ArticlePubMedPMC
- Pieroni, L., & Salmasi, L. (2018). The effect of local economic conditions on maternal health: Evidence from Italy. Health Economics, 27(1), e1-e20. https://doi.org/10.1002/hec.3563ArticlePubMedPMC
- Ramaswamy, A., et al. (2021). Digital literacy and healthcare access among pregnant women in low-resource settings. Maternal Health, Neonatology and Perinatology, 7(1), Article 1. https://doi.org/10.1186/s40748-021-00131-0
- Simanjuntak, M. (2024). Digital transformation in maternal health: A post-pandemic analysis. Health Policy and Technology, 13(1), 100-115. https://doi.org/10.1016/j.hlpt.2023.100781Article
- Smith, L. (2023). Social isolation and maternal outcomes: A longitudinal study of psychological and physical health. Journal of Affective Disorders, 320, 45-52. https://doi.org/10.1016/j.jad.2022.09.087Article
- Sterne, J. A. C., Hernán, M. A., Reeves, B. C., Savović, J., Berkman, N. D., Viswanathan, M., & Higgins, J. P. T. (2016). ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ, 355, i4919. https://doi.org/10.1136/bmj.i4919ArticlePubMedPMC
- Townsend, R., Chmielewska, B., Barratt, I., Kalafat, E., van der Meulen, J., Gurol-Urganci, I., & Khalil, A. (2021). Global changes in maternity care during the COVID-19 pandemic: A systematic review and meta-analysis. EClinicalMedicine, 40, Article 101111. https://doi.org/10.1016/j.eclinm.2021.101111ArticlePubMedPMC
- Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software, 36(3), 1-48. https://doi.org/10.18637/jss.v036.i03ArticlePMC
- World Health Organization. (2020). WHO recommendations on antenatal care for a positive pregnancy experience: COVID-19 brief. World Health Organization.
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader Cite
Cite